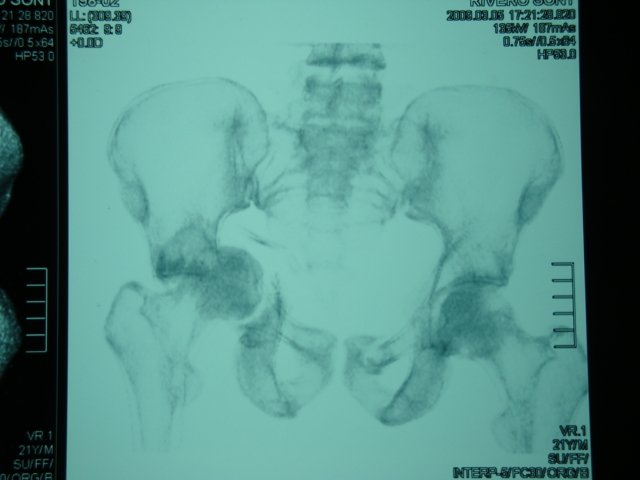
Complex Pelvis Fracture

Pelvis Injuries
Pelvic fractures are often associated with bleeding from rupture of the posterior osteoligamentous complex, sacroiliac dislocation or sacral fracture, as well as possible injury to the sacral venous plexuses or internal iliac arteries, vital vessels that pass through the pelvic cavity. In traffic accidents the most frequent fracture mechanism is a force applied laterally to the pelvis that tends to rotate internally the affected hemipelvis. The biomechanics of the accident (side impact, frontal impact, patient fired, rolled up, etc.), as well as safety measures (seat belts, air-bags, etc.) are important to understand and even anticipate possible injuries.

The Killer Fracture
Pelvic fracture should be considered in all polytraumatized patients, especially if it is associated with hypotension without response (or transient response) to fluid therapy. There is a risk of hemorrhagic shock from massive blood loss that accumulates in the pelvic cavity and/or retroperitoneal space.
The colon, bladder, rectum, or ureters (tubes that carry urine from the kidney to the bladder) may be injured. The most serious thing that can be affected are the arteries inside the pelvis, due to bleeding. There the probability of mortality can be very high.
Some call this injury "the killer fracture" because it is associated with a high probability of mortality. It can be as high as 40 or 50% if it is not treated correctly.


Complex Fracture
In more complex lesions, instability is in both the vertical and rotational planes. There is complete rupture of the posterior ring and the anterior ring can be fixed with both external fixator and anterior plates. Treatment of the posterior arch varies according to the broken portion of the pelvic ring. For fractures of the sacrum and sacroiliac joints, direct posterior percutaneous fixation from the ilium to the sacral body has been described.
This technique presents the risk of being able to injure the lumbar root L5 and the iliac vessels anterior to the sacral body. Transiliac stem fixation may be used in complex sacral fractures. Posterior arthrodesis may also be used. Another possibility is to perform osteosynthesis with plate and screws by anterior and retroperitoneal approach. It is suggested that anterior and posterior internal fixation in unstable fractures is much more effective than external fixation.
Dr. Leopoldo Maizo - Orthopedic Surgeon


Firma diseñada por @themonkeyzuelans, contáctalos vía Discord "themonkeyzuelans#9087"
Great projects from the Steemit community:

- My Fundition campaign: https://fundition.io/#!/@drmaizo/6f88ggj8h

.png)
