DENTAL HEALTH - Is it possible to heal your teeth?
Like most fields of health, dentistry is filled with wall to wall lies.
As the Wellington Chapter of the Weston A Price Foundation, and also through our business Nature Foods, we are often asked questions about dental health.
Knowing this is vast and complex subject, to be honest we have for a long time just refered people to other sources. And that is all this post is - a compilation of good advice from other sources. But Steemit has got a real gap in dental health information and I'd like to put some on the blockchain.

In more recent years the subject has really taken off, more people know about dental cover ups like root canals and fluoride, and are aware that like most mainstream nutrition advice, most mainstream dentistry advice is a dangerous bunch of lies.
Here is a selection of useful articles that explain dental health without all the myths.
Remineralising teeth
We often get enquiries about how to remineralise teeth.
First, go to the website of Ramiel Nagel, author of “Cure Tooth Decay”, which will give you enough information to get started. If you need serious help, it would be well worth getting his book.
http://www.curetoothdecay.com/Tooth_Decay/tooth_decay_overview.htm
To give a very brief summary, tooth decay isn’t caused by sugar coating our teeth, but rather by imbalances in our body chemistry.
So to heal tooth decay, some of the basic requirements are:
A nutrient dense, whole foods, Weston A Price type diet, including:
Bone broths & marrow
Cod liver oil
Butter oil, or lots of good butter
Good quality animal foods, including some raw
Fermented foods
Some people need further specific help to normalise their hormones and body chemistry
A fluoride free, glycerine free tooth cleaner
The last one is important because glycerine coats your teeth, so that they can’t remineralise. Unfortunately, virtually all toothpastes contain glycerine. Other alternatives such as tooth powder are hard to find in NZ. Baking soda is another option.
What Causes Tooth Decay?
A clear explanation of the cause of tooth decay was given by Dr. Albert Schatz in 1972. Dr. Schatz believed that our teeth used minerals in a similar way the rest of our body does. That it utilizes a system of enzymes and chelating minerals. This theory is called the proteolysis-chelation theory. In Dr. Schatz’s proteolysis-chelation theory, it is diet, trace elements, and hormonal balance that are key factors in triggering enzymes and tooth mineral chelation which results in tooth decay.
Why Hasn’t Any Dentist Told Me The Real Cause of Tooth Decay?
In the 1940s the International Association of Dental Research voted that the bacterial theory of tooth decay was correct and silenced the perspective that food and environmental factors were the cause of cavities. With over 30,000,000 root canals performed every year, tooth decay is a billion dollar business.
Rather than focusing on the fact that what you eat is what causes cavities, modern dentistry is narrowly focused on what your bacteria are eating. The false information put out by modern dentistry leads people away from the truth, and away from the real cause and real cure for tooth decay. It is not what you feed your bacteria, it is what you feed yourself that causes cavities. Likewise, special foods can cure tooth decay.
http://www.curetoothdecay.com/Tooth_Decay/tooth_decay_overview.htm
Guide to Holistic Dentistry – Sally Fallon
In addition to his work on nutrition, Dr. Price conducted extensive research into the destructive effects of root canals, detailed in his two-volume work Dental Infections Oral & Systemic and Dental Infections & the Degenerative Diseases.
His conclusions, ignored by the orthodox dental establishment for over 50 years, are gaining renewed acceptance as holistic practitioners are discovering that the first step to recovery from degenerative disease often involves removal of all root canals in the patient’s mouth. The principles of holistic dentistry, based on the research of Weston Price, are as follows:
Eat nutrient-dense whole foods, properly grown and prepared.
Avoid root canals. If you have root canals and suspect that they are causing trouble, have them removed by a knowledgeable dentist.
Avoid mercury (amalgam) fillings. If you have amalgam fillings, have them removed by a holistic dentist who specializes in mercury filling replacement.
Orthodontics should include measures to widen the palate.
When it is necessary to extract teeth, do so in such a way as to avoid leaving the jaw bone with cavitations, which can be focal points of infection.
http://www.westonaprice.org/dentistry/guide-to-holistic-dentistry
The Root Cause Behind Tooth Decay – Dr. John Sorrentino

As a practicing clinical dentist for more than 20 years, I have had many experiences and want to share with you some of my ideas about how to better treat dental diseases. Going to the dentist is an activity that has been engrained in us since childhood. The American Dental Association recommends that everyone see a dentist twice a year. Why is this so, and is it really necessary?
Although dentists today do much more, there are basically only three diseases we treat:
Tooth decay (scientifically called “caries”)
Periodontal (“gum”) disease
Malocclusions, or crooked and overlapped teeth
For all of recorded history, these three diseases have been fairly common in human populations. In dental school, students are taught in detail how to manage and treat these conditions. I was content doing that for a long time, but then I was exposed to some facts that changed the way I looked at disease.
A wise man once said that just because something is common does not mean it is necessarily normal. Since dental disease has been around since the beginning of recorded human history, we have records of disease and treatment going back to the time of the Egyptians and Ancient Babylonians. This makes dental disease common. Unfortunately the paradigm of treating it rather that understanding what caused it became established, and civilization after civilization has had to deal with decay, gum disease and the rest. From the Babylonians, Egyptians, Chinese, Greeks, Romans, Middle Ages and through today, it is a given that decay just happens.
Here is a major truth bomb: NO ANIMAL ON THIS PLANET EATING ITS NORMAL DIET GETS DECAY. Period. Yet we are animals, and we get decay. Connect the dots. See where I am going here?
Sometime in your first year of dental school, they show you a Venn diagram that looks like this:
Tooth decay is the interaction on the teeth between bacteria, which is naturally occurring in the mouth, and fermentable carbohydrates. In a healthy person, nothing else is involved decay. As a dental student, they drill this stuff into your head to the point where it haunts your dreams. What they fail to do is make the case that carbohydrates are not an obligate nutrient for humans. Dentistry has done an excellent job of getting the message out that sugars cause decay. What we have failed to do is get people to understand that starches are metabolically the same currency. The fat phobia that started in the second half of the twentieth century that continues today has only compounded the problem as people have replaced healthy fats with carbohydrates. When viewed this way, the solution is self-evident: Carbohydrate restriction.
Why am I so certain and how do we know this? Several lines of evidence converge to lead to this conclusion.
Clue 1
Back in 1990 when I was a newly minted dentist, I had a friend that was working on a Ph.D. in anthropology and human evolution down at SUNY Stony Brook. Since tooth enamel is the hardest substance in the human body, it is most likely to survive, and my friend spent a lot of time studying it. My friend gave me the understanding that humanity is 2 ½ million years old and gave me a tour of the “skull room” at his school. I was amazed that every single skull in that room was over 10,000 years old yet demonstrated a full complement of 32 teeth with no decay, impactions or gum disease. We had remarked on it but thought no further about it for 20 years.
My friend’s name is Dr. Peter Ungar. He is now the chair of the Anthropology Department at the University of Arkansas, world-renowned experts on dental micro wear and the author of numerous publications on the subject, including a book titled Evolution of Human Teeth, the Known, Unknown, and the Unknowable.
Clue 2
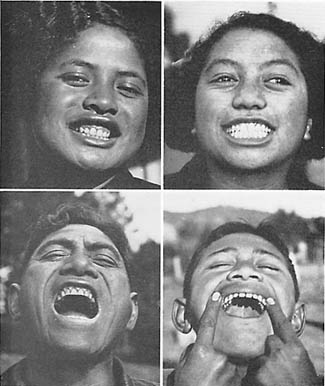
Dr Weston Price’s book Nutrition and Physical Degeneration is a tour de force that documents the results of ancestral diets. Most convincing are his pictures of large families that document healthy teeth in older kids while the younger ones, on a modern diet of rice, wheat flour and sugar (or as he termed it, “The displacing foods of modern commerce”) are crooked and riddled with decay. You can actually tell within a year or two when the family stopped eating a traditional diet. This would also suggest that excessive carbohydrate consumption might be linked to growth disorders that lead to malocclusion and need for orthodontics. Unfortunately for the world, Dr. Price took a few stands in dentistry that made him (not entirely without cause) unpopular. Compounding the problem, his book was published on the eve of World War II. This was a notoriously bad time for science, unless you happened to be working on rockets or jet engines.
More evidence may be found by looking at current populations, such as the Inuit of the far north or the Masai of Africa. While the traditional Inuit diet contains very little plant material and is heavy in fish and sea mammals such as whales and seal, the Masai eat tubers as well as cattle and some dairy, nothing from the ocean. The Inuit have almost no fiber in their diets. The Masai have some but not nearly as much as we are advised to eat, so this does not appear to be the issue. Neither does much sugar, refined or otherwise. No surprise that both groups living thousands of miles apart in completely different climates, but both have perfect teeth.
Clue 3
The work of Dr. Ken Southward and The Systemic Theory of Dental Caries is a somewhat wonk-ish and esoteric work, but it firmly shows that dental decay is the result of a chronic inflammatory response. It also demonstrates that the dental profession is working with an incomplete understanding of what causes decay and the body’s protective mechanisms. Did you know that the parotid gland has an endocrine function and is a dual use gland like the pancreas? Me neither, and I have a degree in dentistry. It is not taught in dental school but to make a long story short, the parotid gland secretes a hormone that helps teeth fight off plaque. Want to guess what blocks that hormone signaling at the level of the hypothalamus? That’s right, sugar! If you read the article you will also have a greater understanding of how fluoride use became prevalent in dentistry and why it may be useful but is generally not needed. I will have more to say about this in the months ahead.
Link these three lines of evidence, and it becomes clear that dental diseases are in fact Neolithic diseases. Modern dentistry is designed to treat these conditions and sees them as somewhat “normal.” I have spent a considerable amount of time and energy trying to convince dentists of our need to change, but you, as a consumer of dental services, are the vanguard of that chance. In the months ahead, I will have plenty to say on these and other subjects in the sphere of dentistry.
http://www.jackkruse.com/dentistry-dr-john-sorrentino-cause-behind-tooth-decay/
Oil Pulling for a Brighter Smile and Better Health – Dr Bruce Fife
The first thing that most people notice when they start oil pulling is an improvement in their oral health. Teeth become whiter, breath becomes fresher, and the tongue and gums take on a healthy pink color. Even problems such as bleeding gums, tooth decay, and gum disease are greatly diminished or completely healed
http://www.coconutresearchcenter.org/article%20oil%20pulling.htm
The teeth in disease – Dr Jack Kruse
Most of you may not know that before I was a neurosurgeon I was a dentist and oral and maxillofacial surgeon. Many people know that Weston A. Price was a dentist too, who was ostracized from organized dentistry for many political reasons. Much of his accomplishments have been largely under appreciated because he was painted as an “renegade” by the American Dental Association and by organized dentistry. Most dental students never learn a thing about him or his work as a result. The paleo community knows about Weston A. Price largely because of his foundation and people like Sally Fallon and the newer generation of young bucks, like future PHd, Chris Masterjohn. When I went to dental school at UCONN, my classmates and I never learned a thing about Weston A Price. We never were told about his work or his books. In the last 25 years, my education has evolved from dentistry to oral surgery, then to neurosurgery, and now to evolutionary molecular biology and it hopefully it will end in Optimal longevity.
My background is different, and kind of gives me a unique view point into medicine, surgery, and aging. Unlike many other paleo practitioners, I look at health and disease a bit differently. If you have read my QUILT, you know that levee one is the top of the heap. The cellular terroir determines all things in biologic terms for the future’s of our cells. Lately, there has been a lot of “discussion” in the blogosphere about macronutrient theories of obesity and the role of carbohydrates, and most of you know that my views on the situation are different then some of these paleo luminaries. Instead of drawing a line in the sand on macro-nutrients, I have chosen to look at the problem through the optic of how our brain accounts for electrons from our food, and how it responds to those signals via the hormonal signals from our hypothalamus in our brain. The main hormone that determines how we partition electrons is leptin as I have laid in my quilt and many of my blogs. Today, we are going to talk about an area that has never been tapped in our community–How might diabetes and obesity begin when we view the problem through an “old” scientific finding that has been largely ignored since it was discovered in 1968.
I’d like to introduce you to John Leonora, Ph.D in endocrinology. He was a medical/dental researcher who like, Weston A. Price, was largely ignored by most of organized dentistry and medicine. He toiled at Loma Linda University, and he recently died in February of 2006. I first heard his name in 1986, when I was a first year dental student at UCONN during a class on the origin of dental caries. Back then, I heard a presentation on a new theory of dental caries based upon a lecture that Dr. Leonora gave in 1983. I became reacquainted with some more of his work from some of my current patients who are 7th Day Adventists and one of my former dental school classmates, Dr. John Sorrentino recently. My 7th Day Adventist friends turned me back on to his work in 2006 and I largely ignored this information again after I read it. I think I never fully grasped the implications of it, honestly. I compiled the articles he wrote, and in 2006, put them in a file cabinet under the tab called the “oralhypothalamus”. Then in October 2011, my old buddy Dr. Sorrentino, from UCONN, sent me an article in a general dentistry magazine to read. As soon as I saw the name, John Leonora, lightening struck my own memories. It was time to synthesize what I remembered from those articles in 2006 and the 1986 talk, and what I now know and write something cogent for you to consider.
Dr. Leonora had some new theories about how dental caries (tooth decay) were caused. He rejected the dogma I was taught in dental school that the acid from bacteria caused demineralization of enamel and dentin in teeth to cause dental decay. He took it much further. He postulated that that dental caries was caused not by bacteria, but caused by inflammation that was due to hypothalamic interruption of hormones that controlled avascular structures in teeth and other endocrine organs. He believed that the parotid gland in our mouth acted just like our pancreas does in our gut. He believed that the parotid gland indirectly controlled the metabolism of avascular structures like dentin, enamel, and the islets of Langerhans that control insulin release in the pancreas. This axis essentially helped the brain sense the initial carbohydrate breakdown in the mouth, and relayed that data to our parotid gland and pancreas to formulate the brain/gut axis response hormonally to this energy substrate. This is why salivation and insulin secretion can often occur before a sugary meal is even eaten. Leptin receptors are also now known to exist in the mouth, gingiva, and on taste receptors.
In 1986, as a first year “dumb ass” dental student, I had no idea how brilliant this man was then. Moreover, how incredibly ignorant the rest of the dentistry and medicine was to his findings that began in the late sixties. Today, I now know about the tremendous accomplishments of Weston A Price, so it comes as no surprise that another dental researcher findings are finding the light of day today. Dr. Leonora found that rats fed a high cariogenic diet (high sucrose diet) had the flow of dentinal fluids completely reversed in their teeth. This reversal of dentinal fluid caused the teeth to become susceptible to decay because it fostered an inflammatory terroir in the tooth. In 1978, he wrote about the systemic role of trace elements in glucose metabolism (Magnesium and Zinc). Remember, from the Gnolls blog post we spoke about how the loss of intracellular magnesium was the first biochemical step in developing diabetes, but not the first quantum effect that causes it. Dr. Leonora found the exact same thing in the hypothalamic parotid axis too. I don’t think this is a coincidence either. Prior to this in 1975, he wrote about the effects of carbohydrates on the hypothalamic parotid gland endocrine axis and how it mimicked the endocrine and exocrine pancreatic physiology. He followed this line of research up with working out how the parotid gland also had dual endocrine and exocrine function like the pancreas. He showed in the earlier 1980′s that dental caries was largely influenced by hormonal fluctuations and not from bacterial acid production to cause disease but from hormonal changes due to a foods carbohydrate load. This hypothesis was largely rejected at the time. Even today, most dentists and physicians are ignorant of this mans work. I knew about it because I listened to his 1983 talk on this at UCONN medical library and my professor pretty much shot it down after I asked him about it. He was quick to point out citing the “accepted research at the time in the literature.” I totally forgot about it until recently.
Mainline scientific theories may have long lifespans, but are inevitably overturned as accumulating evidence renders them obsolete and brings alternative theories to the fore. This happened in physics in 1905 with the advent of the theory or relativity, and it happened 150 years ago in biology, when many diseases did not spontaneously generate but whose etiologies became explainable when germs and viruses become known. It has now happened again today in molecular biology with ROS and antioxidants effects on mitochondria as well. Dr. Leonora’s work was pretty shocking for the early 1980′s scientific community, and I failed to realize its significance until recently as well. My knowledge back then was fairly limited. Today, I am a bit more well rounded and I think his work merits some further attention.
When such a major scientific change in paradigm happens, there is usually a period of significant and often bitter controversy between scientists seeking to hold on to the theories of the older paradigm, and those espousing the newer one. The recent disputes on obesity from Taubes, Guyenet, and Harris come to mind. Often, this is followed gradually by changes in basic thinking patterns and a subsequent long period of fertile discovery. That fertile ground takes many shapes. Today’s post is planting some more of those seeds for you to think about.
It appears that obesity and diabetes development “might begin” in the oral cavity. We know that carbohydrates are first broken down by salivary gland amylase. αamylase breaks down long-chain carbohydrates. Most human amylases tend to be alpha amylases. Both the parotid gland and pancreas share this physiology. It appears the endocrine function of the parotid gland’s acinar cells respond to a releasing hormone of hypothalamus. This ability is only found in the human parotid gland. If the human parotid gland is removed, the hypothalamic parotid axis ceases to work on dentinal flow. Oral inflammation occurs and sets the stage for disease propagation. It appears that this axis is coupled to lingual leptin receptors, and possibly to parotid gherlin levels. This releasing hormone signal from the brain releases a parotid specific hormone that directly effects the flow of fluid in dentin and helps forms teeth and to calcify and re-calcify decayed teeth (with Vitamin K2) to keep them in optimal health. When the process is broken down, dentinal fluid reverses towards the apex of the tooth, and we absorb things from the oral cavity we should not and it causes an inflammatory response. This is precisely how inflammation enters the tooth and jaw to cause inflammation. It also helps explain why diseased teeth show apical abscesses as the inflammation become chronic. It also appears to be the mode of action in how we absorb heavy metals from amalgams and metal dental framework. It further sheds light on why bad periodontal and dental health correlates well with cardiac risk and elevated cardiac CRP and diabetes. It appears the oral cavity is the initial sensory sensor for foods for the hypothalamus as well.
This parotid signaling system is how the brain readies the “avascular parts” of the gut for the onslaught of carbohydrates that will eventually hit the duodenum. The Islets do not have a direct blood supply. They have a portal blood supply much like that of the pituitary gland. It readies the avascular Islets of Langerhans of the pancreas to further deal with a carbohydrate load. It seems to somehow effect the islets portal blood supply and its gene regulation even before the carbohydrates hit the duodenum to signal the pancreas to action. There is research ongoing to see if the parotid gland somehow is involved in the biphasic release of insulin. It also appears that Dr. Leonora discoveries should have illuminated some light on the significance of the hypothalamic parotid gland endocrine axis as it relates not only to dental care, but also to endocrine pancreatic function and the possible development of diabetes and obesity. Sadly this curious finding remains largely unknown by even the most learned neurobiologists and clinicians. I hope this changes soon, because it might just uncover more information to help us help people restore their health.
http://www.jackkruse.com/the-teeth-in-disease/
Could the cause of your illness be right under your nose? – The Healthy Home Economist

Do you ever wonder what compels a person to take and refute decades of “established” research all in the name of helping humanity?
We recently came across a new piece of information about one of our heroes, Dr. Weston A Price.
Many readers of this blog will already be familiar with who Dr. Price was and the gift to humanity his research continues to provide. After all, we couldn’t perform this research now as we don’t have the isolated cultures still intact!
While most of us are now familiar with the research Dr. Price performed with isolated cultures that he highlighted in his landmark book, Nutrition and Physical Degeneration, some of you may not be aware of the research Dr. Price did with embedding root canal teeth under the skin of rabbits. What could have provoked Dr. Price to conduct this study? What could have compelled a practicing dentist to shift his focus to research? Read on…
As a practicing dentist, Dr. Price once performed a root canal on a 16 year old young man. This young man died of a heart attack shortly thereafter. Dr. Price then removed the root canal tooth from the young man who had the fatal heart attack (after he died) and embedded just the tip of one of the roots of the tooth under the skin on the belly of a rabbit.
Two weeks later, that rabbit died of a heart attack. Dr. Price then removed the root tip from the dead rabbit and again embedded the root tip under the skin of a second rabbit. Two weeks later, the second rabbit died from a heart attack. Over the course of many months, Dr. Price took that same single root tip and embedded it under the skin of 100 rabbits. All 100 rabbits died within approximately 2 weeks, all from heart attack.
100 out of 100? All of the same cause of death???
Clearly, realizing that his dental work had caused the death of this young man provoked Dr. Price to shift the direction of his whole life’s work.
Over the course of next 35 years, Dr. Price relentlessly studied the impact that the mouth has on the health of the whole body. He experimented on over 60,000 rabbits (I know, I’m not a fan of animal testing either, but since it’s already been done, let us all learn from the work).
Dr. Price found a correlation between the dental work and whole body diseases. He found that heart attacks are one of the diseases that transferred 100% of the time. But he also found that many other diseases transferred from an embedded root canal tooth to a rabbit. Some of these diseases only transferred 88% of the time. Diseases like arthritis, heart disease, stroke, diabetes, the list is long…
How do we know that the death of this young man deeply impacted Dr. Price? Well, he dedicated one of his textbooks to this young man Donald. Donald Price.
Yes, Weston Price did a root canal on his own son who then died of a heart attack. It’s clear to me as a father that feeling the responsibility for the death of one’s own child would drive a person like Weston Price to make researching the impact the mouth has on the health of the whole body one’s life mission.
We encourage us all to learn from this so the death of a child and the relentless pursuit of the truth over the course of 35 years of research doesn’t go wasted. May we be inspired by this person who was able to take tragedy and redirect that energy into a work so that we could live healthier lives.
http://www.thehealthyhomeeconomist.com/cause-of-your-illness-right-under-your-nose/
Understanding the issues with root canals, part one – orawellness.com

With this article we intend to lay a foundation of the science and research that we have found on the subject of root canal therapy in the hope that having access to this research you will be more equipped to make a more informed decision if you are ever faced with the situation of having to consider having a root canal. We hope this information also assists you along your path to greater oral health and whole being wellness if you already have a root canal as we discuss some of the options you have before you.
We prefer to keep the focus of our work toward bringing you empowering solutions to create positive change in your oral health, so the subject of root canals is tough for us as it’s definitely a consideration of the lessor of two evils…
This is the first of a series of articles on subjects that you, our readers, have asked us to research and share our perspective with you.
We feel compelled to start this article with a strong reminder that stress undermines our ability to have optimal health. Stress literally runs down our immune response. So, if you have a root canal, please read this article lightly. On one hand, we feel the need to share with you what the research suggests. However, please be gentle on yourself and keep your stress levels down. As we are all about bringing positive solutions to light for you, the last thing we want to do is have our work contribute to more stress in your life!
Root canals are one of those subjects that seemingly naturally attract so much attention and create so much controversy. We hope to present the information we have found here on both sides of the issue. That said, we want to disclose up front that we are biased toward the ‘anti root canal’ camp. However, as you will see, this is not a black and white issue. Also, this is going to be a long article so take your time wading through it.
Let’s start by getting a cast of characters from history involved in the discussion.
Weston A Price… Who else?
No discussion about root canals would be complete without looking at the research Weston A Price conducted over 35 years in his exhaustive research. Dr Price studied experimented on over 60,000 rabbits by embedding tips of teeth extracted from humans under the belly skin of the rabbit. He did this to test time and time again how the bacteria from teeth impact the health of the whole body.
In one experiment in particular, Dr Price took a tooth from a person who recently died from a heart attack and embedded the tip of that tooth root under the skin of a rabbit. Within two weeks, that rabbit died of a heart attack. Dr Price then removed the tip from the now dead rabbit and embedded it under the skin of a second rabbit. The second rabbit died of a heart attack within two weeks. Dr Price continued this procedure using the same tooth root with 100 rabbits. All 100 rabbits died of a heart attack within two weeks.
Dr Price found that the only way to stop this progression of the root canal tooth from passing on the disease was to boil the tooth in water for 30 minutes.
How is this possible?
Fact: Teeth are living tissue. And when teeth are alive, they have a flow of fluid through them.
The fact that we need to come to firm grips with here is that although they seem solid, teeth are actually extremely porous. They are filled with tiny tubes, called tubules. These tubules are tiny yet wide enough to house 5 bacteria standing side by side. Think bacterial super highway. It is suggested that the average front tooth has approximately 3 miles of tubules through it (if stacked end to end).
When the teeth are alive, they have blood flowing through them and the blood flow creates flow through the dentinal tubules as well, thus cleansing the tooth. The issue is the fact that a root canal tooth is dead, politically called non-vital. The root canal procedure stops the flow of blood into the tooth which kills the tooth. This makes all the difference as the tooth now has no way to maintain healthy microbial balance within the tubules.
To add insult to injury, the bacterial colonies change when exposed to different environments. When the tooth dies, the environment changes to a low oxygen environment (no fluid flow to maintain healthy environment) which tends to encourage bad bugs capable of producing powerful toxins.
Fast forward 70 years…
Let’s take a look at the research conducted by Dr Boyd Haley, now retired professor of chemistry at the University of Kentucky. To put him into perspective, Dr Haley was one of the first researchers to propose that Thimerosal in vaccines (due to the mercury content) was the most likely toxic agent involved in Gulf War syndrome and autism spectrum disorders.
Dr Haley chose to do his own studies similar to Weston Price’s research on root canal teeth using today’s technology. Dr Haley studied approximately 900 teeth with root canals for their level of toxicity within. He grouped the teeth into three different groups.
Roughly 25% of the root canal teeth studied had bacteria within them which produced toxins that were fairly benign. 50% of the teeth studied contained bacteria within their structure that would challenge a healthy immune system. The last 25% of the teeth contained bacteria which produce toxins more powerful than botulinum (Important note, botulinum is widely recognized as the most toxic substance known to humans). This bears repeating. 25% of the teeth Dr Haley studied contained a toxin stronger than the strongest toxin known to humans…
Starting to see the potential problem?
Side note, although I have not been able to ask him directly, it was told to me that Dr Haley and his wife both had all root canals they had in their mouths removed upon the completion of his studies of root canal teeth.
So, if we take Dr Haley’s research and ponder the implications, it shows us that if a person has one root canal, they have a 25% chance that it’s no big deal, 50% chance that it will cause some trouble and be a source of irritation and aggravation for their immune system, and a 25% chance that it could cause big trouble.
What the research is finding is that certain bacterial strains have an affinity for certain tissues in the body. So, while one bacteria really likes to cause trouble in heart cells, another might prefer liver cells and choose to take up residence there to cause trouble.
The bacterial toxins associated with dead teeth is just one of the issues around root canals. Another issue is the various materials used to fill the pulp chamber of the tooth once the root canal has been performed. Yet another issue is the relationship between the root canal tooth and the bio-energetic flow to the internal organs associated with that tooth.
http://www.orawellness.com/blog/understanding-the-issues-with-root-canals-part-one/
I have a root canal. What are my options? - http://orawellness.com
I wish this were a more fun subject to be discussing. However, we have received so many questions about root canals and positive options available, we want to address this subject for you. For the sake of clarity, we WAY prefer to write about solutions that are purely positive rather than weighing the risks and downsides of various options like when pondering options if a you already have a root canal.
Primary risks with root canals…
In order to really do this subject the justice it deserves, let’s first lay down several primary risks that experts sounding the alarm about root canals bring to light. Last year, we interviewed Dr Robert Gammal on the subject of root canals for our free online event, the HealThy Mouth World Summit. According to Dr Robert Gammal, creator of the movie Rooted which documents the risks of root canals (quick side note, the reference page for the movie has over 250 entries!), the main failures of conventional root canal therapy are:
It is impossible to clean out all the dead tissue from the canal of the tooth. Any dead tissue left in the body becomes gangrenous. The toxins that come out of gangrenous tissue are very toxic to the body and pose a threat to the immune system. Nowhere else in medicine would a physician suggest to leave dead tissue in the body.
It is impossible to sterilize the tooth which leads to the dead tooth having lots and lots of space within it for disease causing bacteria to proliferate. This is the enemy inside the gates of the body.
Dental journals combine these two above issues clearly. “It is now known that complete sterilization of an infected root canal is very difficult to achieve and complete removal of all pulp tissue remnants frequently is not possible.”(1)
Common protocol during root canal therapy is to place antibiotics into the canal. This antibiotic material only gets a short distance into the dentin tubules. The dental literature admits that this type of ‘semi’ application of antibiotics creates antibiotic resistant bacteria.
Substances used to cleanse and seal the tooth are cytotoxic (kills cells) or even carcinogenic (causes cancer).
Ok, so there’s a quick recap of the risks of root canal therapy. Let’s move onto several options someone with a root canal can take to address these potential issues.
Do nothing.
This is always an option. We can choose to care for our immunological health to our best ability, support our health and keep the root canal tooth in place. Keep in mind that despite all the information above, there are many dental professionals who argue that root canal therapy is a safe treatment.
One must reflect that life isn’t over because you have a root canal. Remember that primary to creating greater immunological health is our ability to manage our stress. While diet is fundamental, stress firmly takes its place as the number one factor in creating or destroying immunological health. So, above all else, learn to manage your stress. In fact, if you stress about what to do about your root canal, this is doing a potential double negative. Stop reading, go take a walk in nature with bare feet. Focus on beauty for 5 minutes. Pray. Meditate. Take whatever action (which includes doing nothing by the way) that helps you feel good. This is the number one thing each of us must do to reach optimal immunological health.
Have the root canal retreated using more thorough technologies.
This may be an option for some people looking for solutions. According to Dr Robert Gammal, if we were able to eliminate all the bacteria in the root canal (which using conventional methods is totally impossible), this would be a major step forward. Dr Gammal then states that he thinks we would see a great drop off in the side effects in the disease state from root canal therapy.
The best way we know of to effectively eliminate bacteria during a root canal is to use ozone gas during the treatment. So, if a person already has a root canal, they could choose to have the root canal ‘retreated’ by a dentist who uses ozone gas in their clinic. Different than conventional drills or more recent technology of the use of lasers to cleanse the canal, ozone gas will flow into the dentin tubules and has the ability to eliminate bacteria in the tooth. While we don’t know if ozone gas will completely cleanse the tooth, surely using ozone gas during root canal treatment would be a very wise application of ozone in dentistry to more effectively eliminate disease causing ‘bad bugs’. Here’s a link to an article which has a global database of dentists who use ozone in their practice.
To take it a step further in the right direction, the dentist could reseal the canal using more biocompatible materials in order to avoid the obvious risks from the conventional materials breaking down into dangerous compounds like ammonia, carbon monoxide and formaldehyde. If you really want to go this route, we suggest you have a dental materials blood compatibility test completed. It’s around $300 and you only have to do it once in your life to find out exactly what dental materials irritate your immune system less than others. In this way, you could have materials that are in the ‘less irritating’ group from your biocompatibility test used to seal and fill the canal.
Have the root canal tooth removed.
This is the last option we see possible to answer the question, “I have a root canal. What are my options?” If you choose to have the root canal tooth removed, it is very, very important to have it done properly.
If it’s true that the root canal tooth is a source point for disease causing bacteria to enter the body, then having it removed properly is crucial to insure that the area is cleaned out well after the tooth is removed. Our research suggests that the dentist doing the removal should treat the situation as a surgical procedure. Dr Gammal shared with us in the HealThy Mouth World Summit that he prefers to cut molars into parts so he can be very sure to remove all of the tooth. He shared with us that root canal teeth are very weak and a root can easily break off during extraction. In this circumstance, the dentist has the choice to either leave the piece of root in place, which would be a dreadful choice or go dig around for the tip which doesn’t sound very fun at all.
In our recent other articles on root canals, you may recall that Dr Weston Price embedded a root tip of a tooth that had been root canaled under the skin of a rabbit and provoked the same cause of death that occurred to the human who had the root canal. So, having all the pieces of the dead tooth removed are crucial.
So, it’s best if the dentist approaches this extraction very precisely, treating it as a potential surgical situation.
Another important step sometimes overlooked is the necessity to completely clean out the extraction site after removing the tooth. There is a ligament, called the periodontal ligament, which tends to be a hot spot for infection. The procedure experts have shared with us is they use a rounded burr tip on their drill and clean out the extraction site to remove any infected tissue, including the periodontal ligament.
Of course, if someone chooses to have the root canal removed, the follow up question is, ‘So what are the options to fill the gap?’ We will address this question in an upcoming article in this series which will detail the various options to fill the gap after an extraction and the relative risks and benefits of each option.
http://www.orawellness.com/blog/i-have-a-root-canal-what-are-my-options/
Options if you have a missing tooth

This is the third article in our series addressing the questions we have received around the controversial subject of root canals. In our first article, we focused on the relative risks of root canals that several dentists and doctors have brought to light over the past 100 years. The second article focused on the options a person has if they currently have a root canal. In article two, we essentially address the question, “I have a root canal, what are my options?”
One of the options we discussed in article 2 of this series is to have the root canal tooth properly removed. This article is a natural follow up to article 2 so is going to discuss the options a person has if they have chosen to have a root canal removed. Of course, this article also applies to anyone who is missing a tooth for whatever reason. In this article, we intend to share with you the relative risks and benefits we see with several options a person in this circumstance has.
From our current understanding, we see that a person has 5 options if they are missing a tooth. We will go one by one through them and discuss the risks and benefits associated with each option. Our intent is to assist you in gathering the information necessary to make a wise choice within the larger context of helping you navigate to greater oral health and whole being wellness.
Before we jump into the options, an important consideration is what tooth/teeth in the mouth are missing. We will offer any information we have regarding which options may work better for molars vs front teeth as we walk through these options.
The Principle of Use it or Lose it…
In order to really do this subject the justice it deserves, we need to introduce a principle we find very applicable to the subject of missing teeth. First, we use the term principle to mean a Law that is inescapable. Think gravity. Whether or not we intellectually understand the law of gravity, it has its impact on us every moment. The principle we want to bring to light here we call “Use it or lose it.” Like all principles, ‘use it or lose it’ has many far reaching applications.
For example, we will lose our cognitive ability if not used, so many elderly find enjoyment in exercising their mental faculties through crossword puzzles. If we do not use our muscles, they will deteriorate. If we do not maintain the range of motion of our joints, the body will calcify around the joint to accommodate only the range of motion we regularly use. Our ability to focus our eyesight diminishes unless we exercise our ability to focus our vision at various ranges.
One other example of ‘use it or lose it’ is in maintaining bone density. We are told that bone density will diminish if it is not used. So, the simple movement of a body weight squat to stress the long bones of the legs is an excellent exercise to maintain bone density as we age.
We introduce this principle of ‘Use it or lose it’ in this article specifically because if we do not stress the jaw bone, the density of the jaw can diminish. Chewing on teeth anchored in and around the jaw provides the optimal way to stress/exercise the density of the jaw bones. You will see as we walk through the options below how our ability to stress the jaw bone changes with the various choices one has if they have teeth missing.
Option 1: Do nothing…
The first option we see is to do nothing. As Robert Gammal, one of the experts we interviewed in the HealThy Mouth World Summit, put it in his Aussie accent, “There’s nothing wrong with going ‘gappy’.” While we appreciate Dr Gammal’s willingness to make light of such a situation, having a missing tooth over time may cause some trouble. You see, teeth are ‘place holders’ for one another. So, if a tooth is missing for much time, other teeth that are adjacent to or opposite from (think top to bottom) may shift and change the bite. Yet more proof that we can’t address one part of the body without affecting the whole system, when we have a missing tooth, other teeth can move, impacting the bite of that whole side.
Another drawback of doing nothing is you will not be stressing the jaw bone at the location of the missing tooth thus are at an increased risk of losing bone density at that site. Also, depending on what tooth is missing, doing nothing can compromise one’s ability to effectively use that side of the mouth for chewing. Clearly, another application of ‘use it or lose it’ suggests that we must chew on both sides of the mouth if we want to keep our teeth and jaw bones strong, healthy and functional for us.
On the up side, doing nothing means that you aren’t introducing any other crazy, potentially toxic materials into your system. Another positive to doing nothing is that the area will be easy to clean around, something that is definitely an issue with other options…
Option 2: Traditional bridge work…

Conventional dentistry for years has encouraged traditional bridge work as the ‘go to’ answer to span the gap of a missing tooth. Despite having been used for years, we’re not really keen on this as a viable option for several reasons.
Let’s start by explaining the general idea of traditional bridge work. We apologize up front to any dental professionals if we mis-state any details of the technical aspects. In traditional bridge work, the teeth on either side of the gap are ground down to ‘posts’ in order to attach the fixed bridge.
One main issue we have with traditional fixed bridges is that if either of the two anchor teeth become compromised, you don’t lose one tooth, you lose the whole bridge. Given that the anchor teeth must be compromised by radically stripping away much of the outer tooth structure to prep for the bridge, it will be no surprise to you the number of stories we have heard from our community of this exact situation occurring. Once one of the two anchor teeth become compromised, the person is faced with the situation of losing 3 teeth, essentially an entire chewing capability, on that side.
Another challenge of traditional fixed bridges is the ability to clean under the bridge. You see, you can’t easily floss that area now. So how is someone expected to be able to disrupt and disorganize the bad bugs in the gum pockets all the way around the two anchor teeth? If I had a traditional bridge in my mouth, I know an oral irrigator (think waterpik or hydrofloss) would be my ‘go to’ tool to maintain healthy tissues around those anchor teeth! You simply can’t clean around or under that bridge easily. I can see how oil pulling could be very helpful here.
Another challenge is again looking through the ‘use it or lose it’ principle. The jaw bone under the bridge isn’t going to be exercised.
Yet one more challenge is you are essentially asking 2 anchor teeth to do the work of 3 teeth with a traditional bridge. Asking an already challenged tooth (from the stress of being prepped to carry the bridge) to do half the work of another tooth is asking a lot.
What are the upsides to traditional bridgework? You have a full chewing surface! That’s plenty to celebrate about frankly!
If you have a traditional bridge now, do everything you can to maintain healthy gum tissue around those anchor teeth. You may want to check out our HealThy Mouth System to gain the knowledge and tools to care for potentially deepening gum pockets around those anchor teeth.
Option 3: Implants

I don’t think it will come as a surprise to any of you that we are not fans of implants. I remember hearing about implants many years ago and have felt intuitively all along that something just doesn’t make sense about the idea. With an implant, the dental specialist places a post (most commonly titanium) into the jaw bone at the site of the missing tooth. After they determine that the post ‘was accepted’ by the body, then a crown is placed onto the post.
Several issues surround this subject of implants. Dr Hal Huggins told us in his interview at the HealThy Mouth World Summit that there’s trouble anytime metals in the mouth interact with microbes in the mouth. Dental metals in the wonderfully microbially diverse ‘perfect petri dish’ environment of the mouth tend to compel the bad bugs to adapt and produce atypical toxins. This is big trouble as the body is forced to combat new toxins which can add increased stress to our immune system. While titanium does oxidize more slowly than other dental metals, it is still a metal and as such could be problematic.
There is a much less used material for the implant screw which does offer more promise. Zirconia, the crystal created from super heating the metal zirconium, no longer is a metal so is not going to activate with the bad bugs to produce atypical toxins. I would like to see more research showing how successful zirconia implants are over decades before I would personally consider this a viable option.
Another obvious downside to implants is the cost. Average cost per tooth is 4K to 6K.
The good news about implants is you do activate the jaw bone by chewing on that surface. Thus, you are on the right side of the ‘use it or lose it’ principle. You also will have full functionality of that chewing surface as well as a place holder to encourage other teeth from shifting in the mouth.
Option 4: Composite bridgework…

Here is an interesting alternative to traditional fixed bridgework. Many dentists can build a ‘bridge’ out of composite resin materials (the materials the tooth colored fillings are often made from). The main up side to composite bridge work is that the two anchor teeth aren’t ground to posts. The dentist simply builds off of the adjacent teeth with composite materials to fill the gap.
While not the perfect solution, a composite bridge does offer substantial benefits to other options so far. It’s not metal so no ‘metals and microbes’ issues. The anchor teeth are kept in good condition and not compromised by grinding them to posts. And unlike traditional fixed bridges, if one of the anchor teeth becomes compromised, you can still remove the bridge and keep at least one of the teeth.
Here are a few points why this isn’t a perfect solution… You still have the issue of cleaning around and under the bridge to address. You are also still asking 2 teeth to do the work of 3 teeth. I also wonder how strong these composite bridges are over time. And last, you aren’t exercising the bone under the bridge.
If you would like to look more into this as a solution, search youtube for ‘Carlson bridge’. Dr Ronald Carlson, a biological dentist in Hawaii, has a kit that he sells to dentists to help them have the tools to build a composite bridge. Called the Carlson Bridge ‘winged pontic’, this kit is something your local dentist could purchase at your request to place in your mouth.
If I were missing a front tooth, I would carefully consider having a composite bridge placed to span the gap. It makes sense that these composite bridges could be effective for front teeth, an area that our cultural vanity would make having a tooth missing much more important. I question the long term strength of composite bridge work for molars. On a personal side note, we have a friend who is missing several front teeth from an accident who has a bridge across the whole span. He loves to bless the world with his beautiful smile still! That said, a dentist friend of mine (who I trust his work) just told me that these composite bridges don’t hold up very well. It’s definitely a mixed bag…
(As an added side note, we received a comment from a dentist friend of ours, Dr Paul Rubin, who shared that the Carlson Bridge technology isn’t the only way to go for non-traditional bridgework. You can have a piece milled either by a lab or in office via CEREC technology and have that piece cemented into place. Thank you Dr Rubin for adding this piece to the puzzle!)
Option 5: Removable bridge

The last option we see to span the gap of a missing tooth is some form of removable bridge. There are several styles of removable bridges and they are called by many names. A few of these ‘out of style’ options are removable partials, a flipper, and nesbit.
As their names suggest, each of these options can be removed from the gap. So, it’s easy to clean around. They each would also help to maintain the space to avoid any changes in bite and teeth shifting. As they do sit directly on the gum tissue of the missing tooth, they may also put some demand on the jaw bone thus be working with our ‘use it or lose it’ principle.
There are some possible downsides to removable options. First, they may not fit well and could be uncomfortable. They would require that you be conscious when eating (which isn’t such a bad habit anyway) as they are not cemented into place so could come loose while chewing. You would also have to be diligent with removing it after eating to clean around it as well as mindful where you put it when you do clean the space.
Perhaps the biggest challenge with removable options will be to find a dentist who is comfortable helping you fit one well. Removable solutions are very much ‘out of fashion’ in the high tech, implant frenzy dentistry today. Another potential downside is the material they are made from. We haven’t researched this much, but it seems that dental acrylic is commonly used which isn’t the most benign material.
All this said, if faced with a missing molar, we would definitely look closely into what removable solution would best suit the specifics of the needs to fill that gap.
(As a side note, one reader, made us aware that removable partials should be made from clear acrylic and not look like the image we have in this article. Partials that are colored contain potentially harmful components. Thank you Kathy!)
A possible option 6?
Although we’re generally not fans of hoping that technology will rescue us from any given current mess we humans have created (it shrugs our responsibility to live more responsibility), there is some hope that in the future we will be able to grow new teeth from stem cell research.
http://www.orawellness.com/blog/options-if-you-have-a-missing-tooth/

This content is also posted on our website: www.frot.co.nz
Keep touting it all you want- but I'm NOT getting the Cod Liver oil.
Now can you please post on how to REGENERATE a receding the gum line?
Oil pulling with coconut oil 5 mins twice a day and maybe very gentle brushing with a soft brush
What did you want to say with this article? That some ways to treatment are bad, some are good? Sure thing, it's called medical evolution. Every iteration of treatment gets better and better. All modern medicine will seem like a joke for our descendants. Professional dental clinics, such as https://www.yorkshiredentalsuite.co.uk/treatment/invisalign-leeds-teeth-straightening/, offer the best treatment we can get for now. Don't overcomplicate things. Besides, eating "proper" food is just half of a deal. The world is so complex now, you would never know the real cause of your teeth problems.
Thanks for this valuable information! I didn't know that if you put oil on your teeth, they get whiter.
And talking about the options when you have a missing tooth, I think it all depends on the condition of other teeth. Recently, I got an implant, and I'm happy with it. Before that, I ate a nut, and my tooth fell. It's good that I found an article about how to make a temporary tooth filling. It helped to caution against inflammation.
In case you're curious, it's this - https://www.dental-detective.com/homemade-temporary-tooth-filling-a-how-to-guide/.