Do you know the symptoms of an Acute Myocardial Infarction?
Most cardiovascular diseases are usually the result of an atheromatous pathology, capable of triggering an ischemic event, which may give rise to angina pectoris (for those who mostly call it pre-infarction) or an acute myocardial infarction with or without elevation of the ST segment, based on the electrocardiographic characteristics, which will be discussed later.
To understand a little better, we must initially describe the acute coronary syndrome (ACS) represents an entire medical emergency, and should be diagnosed as early as possible, monitored and treated. Most of these coronary events are usually the result of a rupture of a portion of an atheromatous plaque located near the coronary circulation capable of causing a spasm vessel whose duration will determine the presentation of the syndrome and injury to the myocardium.
Licensed CC BY-SA 2.1 JP. Author: BodyParts3D/Anatomography
Patients with this type of pathology have risk factors that predispose them, such as obesity, sedentary lifestyle, sex, hypercholesterolemia, family history of acute myocardial infarction, diabetes mellitus, hypertension, alcohol and smoking.
Although these events are more frequent in men over 45 years of age, women after menopause have a similarity in the frequency of events and this is due to the loss of production of good HDL cholesterol as a result of the drop in estrogens.
The Human Heart
This noble white organ is located in the rib cage, surrounded by the lungs, and deviated to the left. It fulfills the function of pumping blood to the different tissues of the human body.
The heart is made up of two atria and two ventricles, through which blood flows and reaches the lungs and then allows its exit and distribution, thanks to its ability to propel other organs and tissues, which is why the heart is called a heart pump.
The blood arrives through the venous system, enters the heart through the Right Auricle (AD), going to the tricuspid valve, which allows passage to the right ventricle and finally to the pulmonary artery until it reaches the lungs, where the blood undergoes a process of oxygenation.
Once the blood receives the O2 supply, it goes to the left atrium, passing through the mitral valve and then to the left ventricle, which together with the aortic valve, manages to propel the blood to the different tissues.
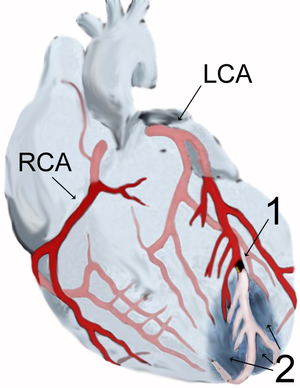
In addition to the heart's chambers, it also has blood supply through the right and left coronary arteries.
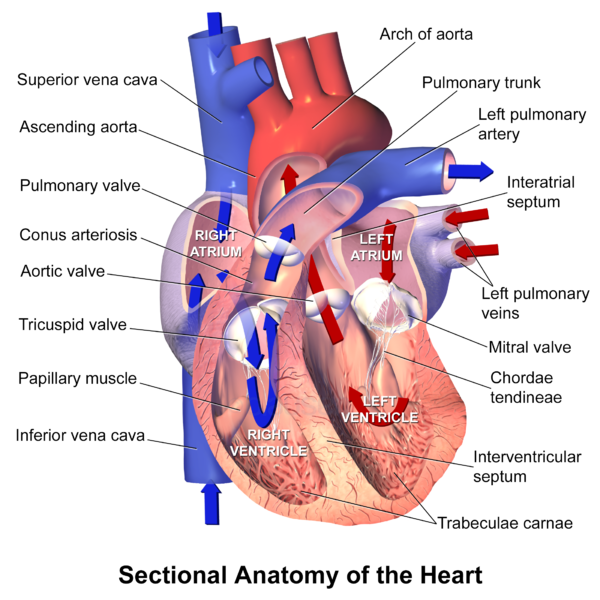
Anatomy of the human heart. Licensed CC BY 3.0. Autor: Blausen Medical Communications, Inc.
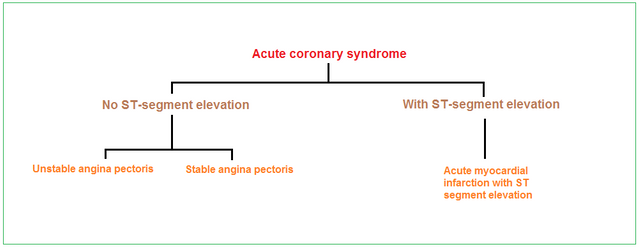
Acute coronary syndrome
This acute pathology, as we have already mentioned, is the product of a vasospasm due to the presence of a thrombus that generates ischemia, and depending on the duration, size of the lesion we will have the presentation of ACS.
Classification
Will be given based on what is observed in the Electrocardiogram.
SCA without ST segment elevation: here we have a subclassification, which refers to the presence of a thrombus in the coronary circulation, which does not completely obstruct the light of the artery. And we have:
While on the other hand we have those ischemic events, where the obstructive lesion will be total, and when performing the electrocardiogram (ECG) we will observe an elevation of the ST segment. In this classification is where we will have:
With the presence of the Q wave, or not Q wave.
Having quite clear the description of the acute coronary syndrome, this post, we will develop and describe the acute myocardial infarction.
Acute myocardial infarction
This pathological entity is the product of prolonged ischemia with sudden interruption of blood supply leading to death and cell necrosis of the myocardium, involving one or more heart faces.
¿What happens physiopathologically?
The individual must have an atheromatous / atherosclerosing disease, which allows the formation of an atherosclerotic plaque in coronary circulation, which due to local stress factors, general rupture of the plaque and detachment of it will generate obstruction of one of the coronary arteries which in this case is total.
These thrombus product of the unstable plaque, originates an occlusion that in some way or another generates a transparietal lesion of the wall of the ventricle of the heart, and in the coronary artery involved and this allows that when performing the electrocardiogram the elevation of the ST segment is observed.
During this process, the release of substances mediating inflammation and platelet aggregation play an important role.
It is important to bear in mind that there are other non atherosclerotic diseases that can cause an acute myocardial infarction, such as thoracic trauma, arteritis, addiction to cocaine and other illicit substances, thromboembolism, and congenital anomalies.
The final result is necrosis of the myocardium, as a result of a total and sustained obstruction of the flow of some of the coronary arteries, leading to the loss of the affected tissue and therefore an increase in the overload of the ventricle.
This is why these two factors, both necrosis and ventricular overload, require cardiac remodelling, which consists of dilation, hypertrophy and finally scar formation.
Clinical Manisfestations
Retroesternal pain is usually abrupt onset, at rest or with physical exertion, of strong intensity.
This pain in most cases is described as oppressive, stabbing, burning, lancinating, persistent, which sometimes despite the administration of nitroglycerin usually lasts, and is not modified, with movements, rest and breathing.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Other associated symptoms; difficulty breathing (dyspnea), coldness, profuse sweating, nausea, vomiting, relaxation of bladder and/or rectal sphincter.
Complications: among the most frequent; acute pulmonary edema, congestive heart failure, cardiac arrhythmias, syncope, cerebrovascular event and cardiogenic shock.
In order to confirm myocardial necrosis or AMI, a good medical history, physical examination, electrocardiogram and laboratory consisting of a cardiac enzyme request must be performed and implemented.
Medical history: basically directed to a good current disease, characteristics of pain, intensity, duration, how it appeared (rest or physical activity), irradiation or not, among others. It is also important to interrogate personal pathological antecedents, if you are diabetic, hypertensive, cardiac and of course to investigate the first line family antecedents.
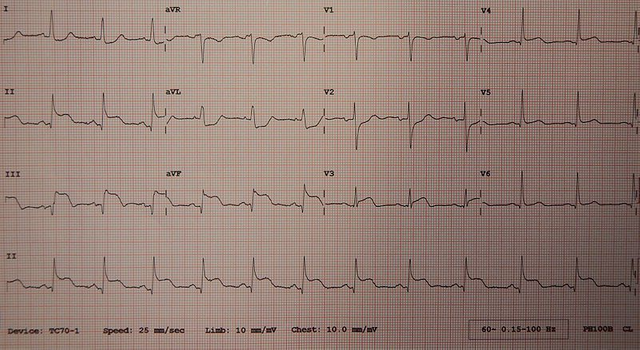
Electrocardiogram
A very useful medical technique, whose function is to record on graph paper the cardiac activity by means of precordial shunts.
The characteristic in this type of AMI cases is to observe the ST segment supra-level in any of the heart faces, and these are:
{kind=link}
Licensed CC BY-SA 4.0. AuthorJames Heilman, MD
Cardiac enzymes
The most specific and sensitive are the quantitative troponins and, failing that, the qualitative troponins, which are indicators of ischemic lesion and cardiac necrosis. They become positive 3 hours after the event and last up to 1 week.
The CPK enzyme (CK-MB), another option but less sensitive and specific, becomes positive a little later the 6 hours approximately and is negative the third day.
Finally and with less specificity we have LDH (lactate dehydrogenase) which is usually elevated in necrosis and tissue damage of any kind.
It is also recommended to request the rest of the paraclinic as is the case of complete hematology, renal function, liver, lipid profile.
Transthoracic echocardiogram
Complementary image study, which is requested 72 hours after the pain subsides and there is no evidence of new changes in the electrocardiogram and is performed in order to determine the degree and extent of damage to the myocardium.
Medical management and treatment
The decision of the treatment that we will give to the patient will be made on the basis of the duration of the pain from the moment it was initiated until its diagnosis. The ideal in these patients is that the diagnosis is made early in order to treat it and avoid the least damage to the myocardium.
If the time from pain to the emergency room and diagnosis is more than 8 hours, you would already have criteria to receive fibrinolysis and treatment to receive will be with oral antiaggregants. In general terms and in summary form.
If we are under the context of an AMI with ST segment elevation and with less than 8 hours of evolution, consider that it is in a therapeutic window to initiate fibrinolysis.
Therapeutic impact therapy
SKR Streptokinase at a dose of 1,500,000 diluted in 100 ml of 5% dextrose or 0.9% physiological solution and passed in one hour, with continuous cardiac monitoring, blood pressure controls, electrocardiogram, and monitoring for signs of bleeding or cardiac congestion.
We must remember that there are situations that contraindicate this thrombolysis therapy.
Absolute contraindications: manifestations of bleeding (previous digestive haemorrhages of less than 3 months) previous cerebrovascular events in the last 3 months, intracranial neoplasms, cranioencephalic trauma of less than 3 months.
The ideal in these patients is early diagnosis and medical treatment to avoid prolongation and expansion of the myocardial lesion. In this way we avoid acute complications such as acute pulmonary edema, signs of heart failure, cardiac arrhythmias and cardiogenic shock.
Some curiosities

{kind=link}
Iker Casillas. Licensed CC BY 3.0
As is well known and currently in the news, Spanish footballer Iker Casillas, 37 years old, with no history of cardiovascular disease, no diabetes, no psychobiological habits, and no family history of AMI, suffered at the end of April of this year, during routine physical training, a coronary event such as Acute Myocardial Infarction, probably secondary to a silent undiagnosed injury that warrants cardiac catheterization.

steemSTEM is a project of the chain of blocks that supports the scientific content in different areas of science. If you want to know more about this wonderful project you can join the server in discord
This article will be published at https://www.steemstem.io/
I hope you enjoyed my content.
Thanks for this! Use to I researched the issue of tissue necrosis!
Now, I'm studying mitochondria which are the main energy delivering units in heart muscles, right? Is it true that the heart relies on glycolysis when there is no high energy demand? What do you think about the keto diet? Might this damage your heart in case of low energy demand due to the lack of sugar?
Thanks and respect
Chapper
Greetings @chappertron, very interesting your question, both the heart, and other vital organs such as the brain, which has the highest demand for glucose for its proper functioning. This diet consists of a low-carbohydrate diet rich in fats and proteins, similar to a fast which in the end leads to a ketonic state, which is a product of this load of protein and fat at liver level are degrade to ketonic bodies that will later be used as the fuel to replace so say for the cells.
This type of diet has been highly recommended especially for patients with metabolic syndrome, dyslipidemias and prediabetes. Its beneficial effect on the heart is that it decreases the accumulation of bad cholesterol in the walls of the great vessels, which predispose to coronary events such as angina or heart attacks.
Usually they are a strict diet regime, they are usually managed by nutritionists, it is not so much my strong and I am not very good for safe diets :) hehe. I always recommend eating healthy balanced and exercising. Thank you always for reading my articles and your support. Happy weekend.
A happy weekend also for you!
Taken together you see no server health risk by triggering ketosis!?!
What if somebody eats mostly fish and healthy fats? Could they then do the keto without amassing the bad cholesterol?
Greetings @ alexander.alexis I always recommend a diet rich and balanced the pestado is a source of protein with low fat very beneficial for health, but as I said earlier dietary regimens are handled by nutritionists. Thanks for reading the article
Congratulations! I just stopped by to say that your post has been selected as a daily Featured Post of my personal curation project! You can find the daily Featured Post HERE.
I upvoted your contribution and I put it on the list because to my mind your post is what I call a quality content!
I am @miti, a manual curator that shall make available all his Steem Power to authors deserving of support. Let's make STEEM great again!
Have a nice day and keep up the good work!
Thank you very much @miti
It's a pleasure!
This post has been voted on by the SteemSTEM curation team and voting trail. It is elligible for support from @curie and @utopian-io.
If you appreciate the work we are doing, then consider supporting our witness stem.witness. Additional witness support to the curie witness and utopian-io witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Thanks for having added @steemstem as a beneficiary to your post. This granted you a stronger support from SteemSTEM.
Thanks for having used the steemstem.io app. You got a stronger support!
Thank you steemstem
Hi @anaestrada12!
Your post was upvoted by Utopian.io in cooperation with @steemstem - supporting knowledge, innovation and technological advancement on the Steem Blockchain.
Contribute to Open Source with utopian.io
Learn how to contribute on our website and join the new open source economy.
Want to chat? Join the Utopian Community on Discord https://discord.gg/h52nFrV
thank you utopian-io
Valiosa información Dra. Gracias pro el tiempo empleado para brindarnos detalles sobre esta compleja enfermedad. Saludos, gusto en leerla nuevamente