Nephritic Syndrome in Pediatry
Being already in the 5th year of my career, and my 2nd year of internships, things are not being as easy as I expected, but not for the reasons one would expect; as I said in the heading, the constant lack of the most basic public services is making all aspects of my life quite difficult. However, having previously downloaded several books helps, although I cannot find out about the most recent updates, and the lack of electricity leaves me with few things to do besides studying. It was during one of those nights, reading from my Tablet and writing my summaries literally by candlelight, that it occurred to me to study in another way, when the electric service would allow me to: write articles about the topics I needed to study, with my characteristic style. Nothing innovative, I know, but useful and entertaining, for me and I hope for you.
The first articles will deal with topics related to pediatrics, the area in which I am currently in, and one of my favorites; internal medicine on a small scale and with more challenges, basically. Focusing on today's article, I will talk about a relatively common syndrome that can easily be confused with other pathologies: the Nephritic syndrome.
Nephritic Syndrome in Pediatry
Kidney diseases can be easily confused among them; although the kidneys have a good number of different parts that can be affected independently, the symptoms are often similar, and the diagnosis is almost always based on laboratory tests. Perhaps this is why one of my role models (more in terms of preparation and knowledge than in the treatment of patients), Dr. Gregory House, is a nephrologist; with the character a kind of Sherlock Holmes with a medical degree, it is to be expected that his specialization is one in which the final diagnosis is often a difficult-to-decipher mystery.
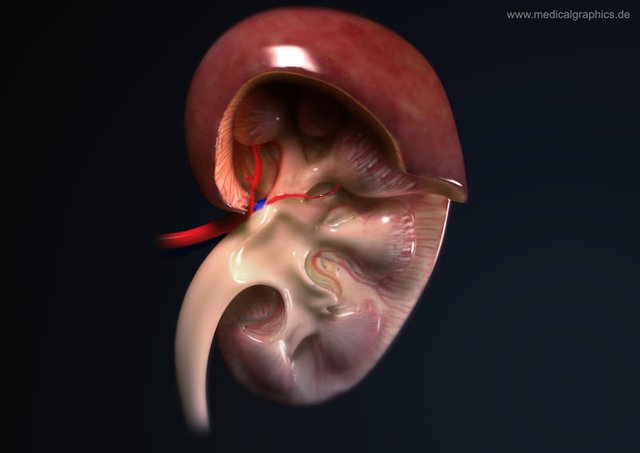
One of these diseases is the Nephritic Syndrome, a condition that, although has a set of specific symptoms which I will explain later, may have a difficult cause to pinpoint. This syndrome is defined as a defect in the glomerulus, which is basically a cluster of capillaries (small arteries) surrounded by an outer semicircular envelope called the Bowman's Capsule, which is found in the nephrons (basic functional unit of the kidneys). It is in the glomerulus where the purification and filtration of the blood occurs, and the first stages of the process of urine formation based on the substances that are eliminated. The glomerulus, together with Bowman's capsule, constitute the so-called Renal Corpuscle, which is the basic filtration unit of the kidneys.
The nephritic syndrome usually has an acute onset, and is characterized by the triad of hematuria (blood in the urine), edema (swelling caused by fluid accumulation), and high blood pressure, although it is usually accompanied by other symptoms, usually caused by inflammation of the glomeruli. However, it is important to bear in mind that this syndrome does not always occur in a complete form, so to speak, and in fact, the term "nephritic syndrome" is currently falling into disuse in some countries, being replaced by the underlying pathology causing the symptoms suffered by the patient, such as glomerulonephritis (inflammation of the glomeruli commonly caused by bacterial infections), or by systemic autoimmune diseases such as Systemic Lupus Erythematosus. That is why the terms of nephritic syndrome and acute glomerulonephritis are often used interchangeably, although it is true that the nephritic syndrome may have other etiologies, and may not always present the same symptoms, since, ultimately, they are two different diseases.
This syndrome is the most common kidney disease in children, especially in those of school age with predominance between 6 and 7 years, and is usually associated with glomerular nephropathies. The most common cause is an acute post-streptococcal glomerulonephritis, that is, due to an infection by streptococcal bacteria, usually by group A beta-haemolytic streptococcus that produces an infection in the pharynx or skin, which then affects the glomerulus. The second most common cause is an autoimmune disease known as IgA Nephropathy (by immunoglobulin A) in which an anomalous accumulation of the antibody immunoglobulin A in the glomeruli causes an inflammation, and the third most common cause is Systemic Lupus Erythematosus, another autoimmune disease. In addition to beta-hemolytic streptococcus, other agents have been associated with acute glomerulonephritis, such as Staphylococcus aureus, mycobacteria, Epstein-Barr virus, cytomegalovirus, and parasites such as Plasmodium, Toxoplasma gondii and Trypanosomes.

{kind=link}
Drawing of a glomerulus, inside the Bowman Capsule.
Regarding the physiopathology, the most common element in the nephritic syndrome, as I said previously, are lesions in the glomerulus, caused by an infiltration of immune cells, mainly leukocytes (white blood cells). This causes an inflammatory reaction that damages the walls of the glomerular capillaries, allowing erythrocytes and red blood cells (main components of the blood) to escape into the urine, causing several hemodynamic alterations that decrease the filtering rate in the glomeruli, causing oliguria (decrease in daily urine volume), because less urine is produced due to problems with blood filtration, and causing a system called Renin-Angiotensin-Aldosterone to activate, producing an increase in the blood pressure. In addition to this, there is an increase in the permeability of the glomeruli, causing the red blood cells and the proteins found in the blood to go out in the urine, and to increase the urea and creatinine, toxic substances normally expelled through urine, which are then reabsorbed into the bloodstream.
Among its symptoms we have already highlighted hematuria, the most common clinical finding and that in more than half of cases is usually visible to the naked eye. When the syndrome is caused by a bacterial infection, the hematuria appears 1 or 2 weeks after an infectious process in the pharynx or tonsils, and 3 to 4 weeks after a skin infection. There is also arterial hypertension, a consequence of the retention of fluids and sodium and the secretion of renin by the kidneys, edema mainly localized in the face, eyelids and extremities and that occurs predominantly in the morning, proteinuria (presence of proteins, such as albumin, in urine), oliguria due to fluid retention, and in severe cases it may cause renal failure.

{kind=link}
Classic example of edema caused by nephritic syndrome
For its diagnosis it is important to inquire about the existence of previous infections or autoimmune diseases such as lupus, and the family medical history should be investigated in search of a history of nephropathy or consumption of drugs or medicines that may have damaged the kidneys. In addition to this, it is important to ask about the appearance and color of the urine. In the physical examination the presence of edema, blood pressure, and signs that may indicate the existence of renal failure must be assessed, just as the pharynx should be examined for signs of previous infections. The laboratory tests are of great importance in order to reach a concise diagnosis, the main one to be performed is the analysis of urine where red blood cells and proteins will be present in generally moderate amounts, and if there is a massive proteinuria, can lead us to think that the etiology is an autoimmune disease. The blood electrolyte and biochemistry studies are also essential; sodium will be low, as will albumin and proteins, while urea, creatinine, and urea nitrogen will be elevated. Finally, the imaging studies can also be useful, such as a renal ultrasound in which the kidneys will be inflamed and hyperechoic.
It is necessary to make a differential diagnosis between the nephritic and nephrotic syndrome, due to the similarity between some of its clinical manifestations. The nephritic syndrome produces a decrease in glomerular patency, has a higher incidence between 5 and 15 years of age, usually occurs after a cutaneous or pharyngeal infection and with a sudden onset, and its clinical manifestations, such as mild to moderate hematuria and proteinuria, hypertension, and mild edema, are related to the decrease in glomerular filtration rate, fluid retention, and the increase of nitrogen compounds in the blood. The nephrotic syndrome, on the other hand, causes an increase in glomerular patency, it is more common in children under 5 years of age, its onset is progressive and there is usually no history of previous infections. The clinical manifestations are different; there is only proteinuria (without hematuria) which is usually massive, there is no arterial hypertension, the edema is severe and can spread to the abdomen (anasarca), there is hyperlipidemia (increase in lipids in the body), and its symptoms are related to the large loss of plasma protein.
There is no specific treatment for the nephritic syndrome, the measures to be taken are symptomatic and supportive, aimed mainly atsolving hypertension and edema. Glomerulonephritis, which is the most common etiology, is usually temporary and reversible, although it can sometimes worsen and cause chronic renal failure. At ambulatory level absolute rest should be recommended for 3 to 5 days as well as a diet low in sodium and protein, in addition to limiting water intake; this if the syndrome and its symptoms are mild. If, on the other hand, the patient has significant edema, severe hypertension, a significant decrease in urinary output and/or severe haematuria, it must be hospitalized. In addition to rest and diet, a pharmacological treatment should be started, using diuretics such as furosemide, hydralazine and nifedipine for high blood pressure, and in forms of rapid progression, corticosteroids such as dexamethasone can be used to decrease the glomerular inflammation. If its etiology is infectious, antibiotics such as penicillin are used to eliminate the causative agents, and in severe cases, or if there are important electrolyte alterations, dialysis should be indicated.
{kind=link}
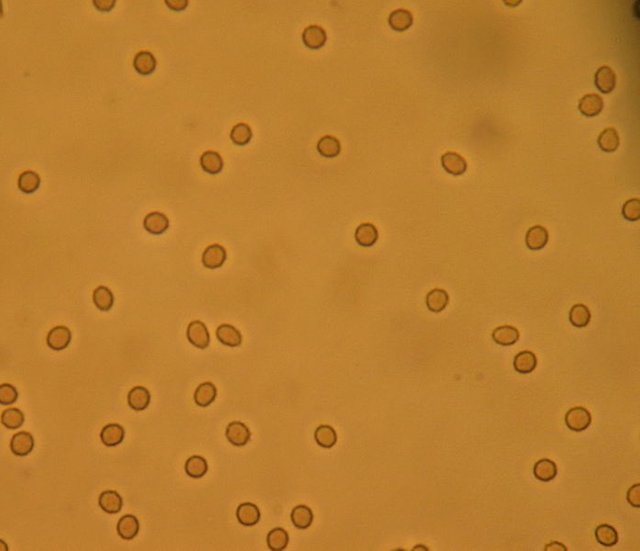
Microscopic view of the hematuria.
Finding urine in the blood can be a dramatic occurrence, and understandably, it can be thought to be due to a serious illness with lasting consequences, but as we can see, this is not always the case. The nephritic syndrome, in most cases, does not endanger the life of the patient and its symptoms are relatively mild compared to the nephrotic syndrome, about which I will speak in a future article. With this, we can realize that in medicine, the severity of the disease is not always related to the symptoms (except in the area of surgery, injuries and injuries are usually as serious as they appear), so you do not always have to be frightened when presenting some apparently serious sign or symptom; it may be something that does not even require treatment.
References:
- Nephritic Syndrome – An Overview
- Nephritic Syndrome – Pediatrics in Review
- Pediatric Nephritis – Medscape
Let me first say that I am sorry about the disruption in your life and the difficulties you face in carrying on every day activities. I admire your determination to overcome obstacles. Then, on to the meat of your article.
The headline caught my eye because of the peculiar history of my family. While none of us has suffered from nephritic syndrome, we do have an unusual incidence of autoimmune disease. This includes pediatric and adult rheumatic fever and adult systemic lupus. As you know, (and as you suggest in your article) both diseases (that is, streptoccocus/rheumatic fever) can be associated with glomerulonephritis. I find it interesting that both diseases have not attacked the kidneys in my family, although cardiac and CNS involvement have been present. I think tracing the specific genetic profile that increases susceptibility to these diseases, and then fine tuning that profile to describe particular areas of vulnerability, might be a way forward to preventing much disease and disability in the future.
The question to be asked: why the heart and not the kidney? Why the brain and not the kidney? At this point I think most doctors consider it a matter of random chance when they ponder which organ system might be affected by these diseases. If science could offer more specific information (about genetic susceptibility) perhaps we could anticipate where damage might occur when these diseases strike.
Of course, I'm not a doctor, or a scientist. Just a person making observations from personal experience. As such, I'm grateful to you for your clear language and easy-to-follow discussion.
I hope your personal circumstances improve.
Thanks, I'm glad you liked it! And you're quite right; there's a lot of research going into DNA engineering just for that purpose you mention. When people hear that term they immediately think about scientists wanting to create super humans, or changing the genes as to breed people of a predetermined race or appearance. However, the real goal behind genetic engineering is that - to eliminate all genetic diseases.
Posted using Partiko Android
Thank you for that answer. Several people who blog on SteemSTEM are doing that kind of research. I have been following it closely.
I'm glad to see you have access to the Internet tonight.
Hope there is peace in your life.
May I ask, who are those people? I would love to read more about the subject!
And indeed I've had relatively stable internet access this week, now I just need the time to post lol
Posted using Partiko Android
Here's a related one from @scienceblocks, and another one. @chappertron ran a whole series on mitochondria and epigenetic influences. Here's and early one, and another one (in German!!)
These may be tangentially related, but they draw a direct relationship between disease, cell biology. I think both writers are brilliant. Also gracious. I'll be following you :) Already tweeted out your article.
You remember me to translate them!
Thanks
Posted using Partiko Android
@chappertron:Es tut mir leid 😔
I was tired last night and the German ones came up first. Fresh with energy this morning, I have found some of the English and am referencing them. Much work to translate, I know 😃
No trouble! It's weekend ;-)
Thanks a lot man, I'll make sure to check them out!
Posted using Partiko Android
@mike961: I found some in English, written by @chappertron. He often translates his articles. Here are a few:
https://steemit.com/steemstem/@chappertron/how-to-live-healthy-part-1-what-are-caloric-restriction-mimetics-crm
https://steemit.com/steemstem/@chappertron/how-to-live-healthy-part-5-what-should-i-do
https://steemit.com/steemstem/@chappertron/how-to-live-healthy-part-4-how-can-i-get-to-the-truth
https://steemit.com/steemstem/@chappertron/how-to-live-healthy-part-3-is-there-an-interplay-between-crm-autophagy-and-telomeres
https://steemit.com/steemstem/@chappertron/clean-up-your-cells-the-best-protection-against-aging-cancer-alzheimer-s-disease-and-co-5-autophagy-vs-mtor-how-can-i-optimally
Looks like I have some reading to do this afternoon! While right now my main interests are topics related to surgery (the service I'm currently serving under, since a couple of weeks ago) I'll always dedicate some time every week to read a bit about genetics and hereditary diseases, I find them really interesting. Thanks for the links again!
Posted using Partiko Android
This post has been voted on by the SteemSTEM curation team and voting trail. It is elligible for support from @curie and @utopian-io.
If you appreciate the work we are doing, then consider supporting our witness stem.witness. Additional witness support to the curie witness and utopian-io witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Please consider setting @steemstem as a beneficiary to your post to get a stronger support.
Please consider using the steemstem.io app to get a stronger support.
Hi @mike961!
Your post was upvoted by Utopian.io in cooperation with @steemstem - supporting knowledge, innovation and technological advancement on the Steem Blockchain.
Contribute to Open Source with utopian.io
Learn how to contribute on our website and join the new open source economy.
Want to chat? Join the Utopian Community on Discord https://discord.gg/h52nFrV
Congratulations @mike961! You have completed the following achievement on the Steem blockchain and have been rewarded with new badge(s) :
You can view your badges on your Steem Board and compare to others on the Steem Ranking
If you no longer want to receive notifications, reply to this comment with the word
STOPTo support your work, I also upvoted your post!
Do not miss the last post from @steemitboard:
Vote for @Steemitboard as a witness to get one more award and increased upvotes!
Nice article (I learned a lot, as this is far from my field!). On different footings, the situation is Venezuela is really terrible, seen from here. Is there any hope to see things improving?
By the way, do not hesitate to use
for the images. This will make them nicely viewable on steemstem.io as well! By the way, I also think that you forgot to close a “boldface” environment… this leads to issues on steemstem.io.
Whoops, looks like when I edit the article in here it's also changed in steemstem.io, didn't know that. I guess I need some tips, I can't seem to make my images appear on both sites at the same time, the markdown code is different. Is there a tutorial or something somewhere? :(
Posted using Partiko Android
And as for my country, to be honest, I don't how things could improve in the short term. It would take quite a few articles to explain the entire political situation , which is actually quite interesting, but in short, things are at a stalemate right now, and unless exterior force is used (a military intervention by the US and its allies) things probably won't get better, because the political opposition still believes that the government will leave peacefully, when they have shown at every opportunity that they would rather literally kill the entire population if that means they would keep their power.
Maybe I'm too much of a cynic, but I've learned to never get my hopes up in here, lest they get crushed and I end up depressed for months. Our only real hope for change is to leave the country, which I expect to do in a couple of years, most likely. But again, all this is a really short simplification of the current political status, if you're interested I could gladly explain some more on discord. And don't even get me started on the economy...
Posted using Partiko Android
This is fine. I already got fragments of the situation here and there and there is indeed no way to summarize it in a few words. it is more a conversation to have with drinks.
I really hope things will change for you guys, but I agree I do not see how at the moment.
Hello, thanks for the article.
I have a question about kidneys. I drink up to 10 cups of green tea a day (I brew it, again and again, to remove all the active substances and to reduce the caffeine content). My question is now: By your profession, would you recommend this or would you rather recommend smaller quantities?
Many Thanks
Chapper
Thanks @chappertron! I would personally recommend you lower your intake a bit, not because of its caffeine content which is indeed probably removed by the brewing, but because drinking excess liquid, be it tea or simple water, basically overworks your kidneys, leading to a higher probability of suffering from renal failure and electrolyte imbalance. Also, while it may not have caffeine anymore, its sodium content may eventually cause kidney stones.
Posted using Partiko Android
Hey there, thanks for the response.
10 Cups are approx. 2.5 L! Which amount of water would you recommend per day?
You may have heard that the recommended amount is 8 glasses of water, equivalent to 2 liters per day. However, truth is, not only is that amount slightly exaggerated in most cases, but everything you eat has a water content which counts for the daily water intake total.
While it's important to always stay hydrated, too much water can be harmful to the kidneys. Therefore, it's recommended to only drink water when thirsty, and it should be enough to stay hydrated. However, there's no problem if you drink some tea - or any other beverage - when you're not thirsty, just don't overdo it.
In short, if you lose a lot of liquid daily, say, if you're an athlete who sweats a lot, 2.5 lt may be a normal intake. But if you don't lose a lot of liquid, either via sweat or by constant peeing, that amount is a bit excessive, and I would recommend you to lower it by a liter or so, as to not overwork your kidneys.
Posted using Partiko Android
👍
Posted using Partiko Android
With the great strides in organ replacement research, I'm hoping that complex organs like the kidneys will soon be successfully grown in the lab.
Enjoyed your post.
Namaste, JaiChai