ORAL MANIFESTATION OF SYSTEMIC DISEASES #RENAL DISEASE
Dear reader, welcome to my blog.In my previous posts I started discussion on oral manifestation of systemic diseases where I highlighted the effects of vitamin deficiency and Diabetes mellitus on oral tissues. In these posts, I also pointed our attention to the fact that,
The mouth is the gate way to the body. That, The mouth is like a mirror that reflect what goes on within our body's organs and systems.The oral cavity (mouth) plays many critical roles in physiologic processes such as, digestion, respiration, and speech and this makes it an important anatomical structure in the body. It is also unique for the presence of exposed hard tissue (teeth) surrounded by mucosa. However, a wide array of systemic diseases, encountered in internal medicine has manifestations in the oral cavity. It is important to state that most of these oral manifestations should alert us as individuals and also the dental practitioners to the possibility of concurrent systemic disease or latent systemic disease that may develop subsequently.
Today I will be taking it further by telling us about oral changes that occur in renal disease. Now lets set the ball rolling!
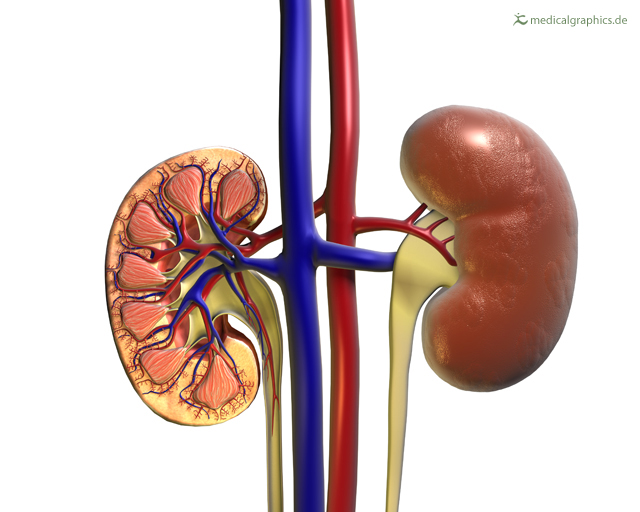
The Kidney
The kidneys are two bean-shaped retroperitoneal organs .The kidneys are very important and serve functions such as;
- Filtration and excretion of metabolic waste products (urea and ammonium)
- Regulation of necessary electrolytes, fluid, and acid-base balance
- Stimulation of red blood cell production. They also serve to
- Regulation of blood pressure via the renin-angiotensin-aldosterone system, controlling reabsorption of water and maintenance of intravascular volume.
- Glucose and amino acids reabsorption and
- Hormonal functions via erythropoietin, calcitriol, and vitamin D activation.
However when there is loss of kidney functions as a result of several primary renal diseases or systemic diseases with renal involvement, the result is End Stage Renal Disease(ESRD). End Stage Renal Disease manifestations involve almost every system of the body, in a clinical condition known as uremic syndrome which is characterized by a marked alteration of water, electrolyte, and acid-base homeostasis, as well as retention of uremic toxins within the body.
ESRD is a condition that is incompatible with life, unless the patient starts chronic dialysis treatment or kidney transplantation. Diabetes mellitus is also an important risk factor for ESRD because about 90% prevalence of DM has been reported in renal disease patients, either on dialysis or with a kidney transplant.
There are more than 30 different systemic signs, symptoms, or oral lesions associated with uremic syndrome and kidney transplant that has been reported in medical literature.However, because of the exigences of time and limited space I will only talk about the followings;
- uremic fetor
- xerostomia
- pale mucosa
- uremic stomatitis
- candidiasis
Uremic fetor
The most prevalent are uremic fetor and unpleasant taste.Uremic fetor was associated with discoloration in the mucosa, and xerostomia.Uremic fetor occurs as a result of a high urea concentration in saliva, and its ensuing conversion to ammonia. Additional causes are increased phosphate and protein concentrations, and changes in saliva pH, which might explain a metallic or unpleasant taste.
Xerostomia in ESRD
Dry mouth in ESRD patients is a multi-factorial phenomenon. This may be due to water restriction in the body, low saliva flow, or fibrosis and atrophy of the major salivary glands parenchymal. Also mouth breathing and medication use in the treatment of the disease has been implicated.
A major risk factor for candidiasis, dental caries, periodontal disease, and bacterial infections in a ESRD/DM patients is Xerostomia because of the lost of protective action of saliva.
Xerostomia is also associated with loss of taste . A higher prevalence of oral manifestations and gingival calculi has been described in ESRD patients with xerostomia.A possible association exist between dry mouth and poor glycemic control in hemodialysis patients.

{kind=link}
Mucosa palor in ESRD
Mucosa pallor is explained mainly by anemia, a multi factorial complication in the ESRD patient caused by:
- erythropoietin and folic acid deficiencies,
- inhibited erythropoiesis,
- shortened erythrocyte life span,
- hemolysis and hemodialysis complications
Other features of ESRD
- Dry- fissured lips, saburral tongue, and candidiasis.
- Saburral tongue is caused by:
- Retention of desquamated epithelial cells and dead leucocytes on filiform papillae and by volatile sulphur compounds produced by anaerobic bacteria on the tongue surface almost always the same as those found in the sub gingival plaque.
- Saburral tongue has also been described as filiform papillae enlargement, with bacteria accumulation due to factors such as a water-restricted diet, low saliva flow, poor oral hygiene, and even the emotional condition of the dialysis patient.
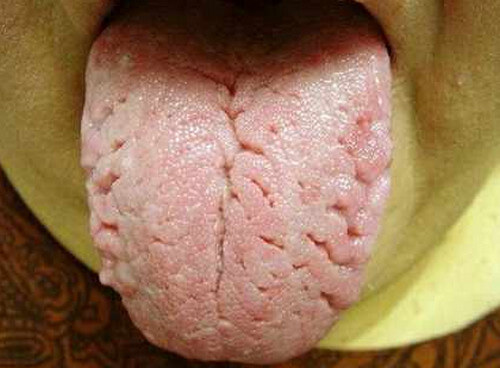
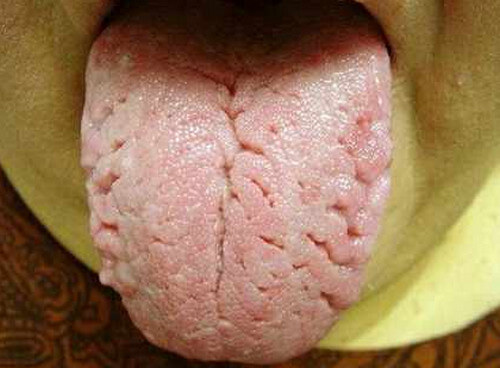
Fissured tongue(cracks and grooves)
source
{kind=link}
Immunocompromised and fungal infections
The causes of the immunocompromised condition of the dialysis patient are uremia, malnutrition, dysfunctional cellular immunity. Immunocompromise increases the risk for opportunistic Candida specie infections.Other known risk factors for candidiasis are xerostomia, low saliva flow, total dental prosthesis, poor oral hygiene, age, and diabetes.

Petechiae, echymosis and mucosa ulcerations
Aggregation of platelet is usually altered in uremia which, coupled with heparin and other anticoagulants used in hemodialysis, predisposes patients to ecchymosis, petechiae and hemorrhages in the oral cavity.
Uremic stomatitis is a localized or generalized burning oral mucosa erythema, with erythematous areas covered by a greyish pseudomembranous exudate which on removal, leaves an intact (type I) or ulcerated (type II) mucosa.
Uremic stomatitis can also be seen as white plaques on the dorsum of the tongue and vestibular mucosa known as hyperparakeratotic uremic stomatitis which often coexist with Candidiasis.
It has been considered to be a reaction to tissue irritant possibly ammonia compounds derived from urea hydrolysis by salivary urease, whenever saliva urea concentration exceeds 180 mg/dl.

{kind=link}
In conclusion, oral health is a major component of systemic health and so effort must be made to limit the impact of systemic diseases on oral health.
Thank you for reading.
This is a test comment, notify @kryzsec on discord if there are any errors please.
Being A SteemStem Member